
Acupuncture & Dry Needling: So What Is The Difference?
The short version
Dry needling and acupuncture use the same needle, target the same tissue, and produce the same physiological response. The difference is that acupuncture has been doing it for over two thousand years, within a system sophisticated enough that it takes four or five modern neuroanatomical concepts working together just to approximate what classical medicine described as a single unified framework. Dry needling is one technique. Acupuncture is the system it came from.
The clinicians most associated with developing dry needling as a distinct practice had prior acupuncture training. Chan Gunn, whose work in the 1970s forms much of the foundation of modern dry needling, was working explicitly from an acupuncture framework and later dropped any reference to that training from his public narrative. That flexibility is the system working exactly as it should.
The borrowed tool
You'll encounter no shortage of explanations from the physical therapy world attempting to draw a line between what they do and what we do. "We base this on Western anatomy." "Acupuncturists just move Qi." "Acupuncture points are arbitrary."
The body doesn't care what you call your technique or what you call the tissue you're treating. It simply responds to stimulus. In the case of dry needling, or “Ashi” and “trigger point acupuncture”, as we've called it for centuries, a needle creates a mechanical stimulus that prompts a trigger point to release. On that narrow point, we agree.
All dry needling is Ashi acupuncture, but not all acupuncture is dry needling. Dry needling is defined by a single application: the use of a solid filiform needle to release a trigger point, an irritable, contracted nodule of myofascial tissue that generates referred pain. This is one technique among many that acupuncturists have employed for centuries. Western practitioners extracted that technique, repackaged it under a new name, and positioned it as the rigorous, anatomy-based counterpart to a medicine they tend to relegate to stress relief and emotional wellness.
"That distinction is semantic, not scientific."
The needle is the same. The tissue target is the same. The neurophysiological mechanism is the same.

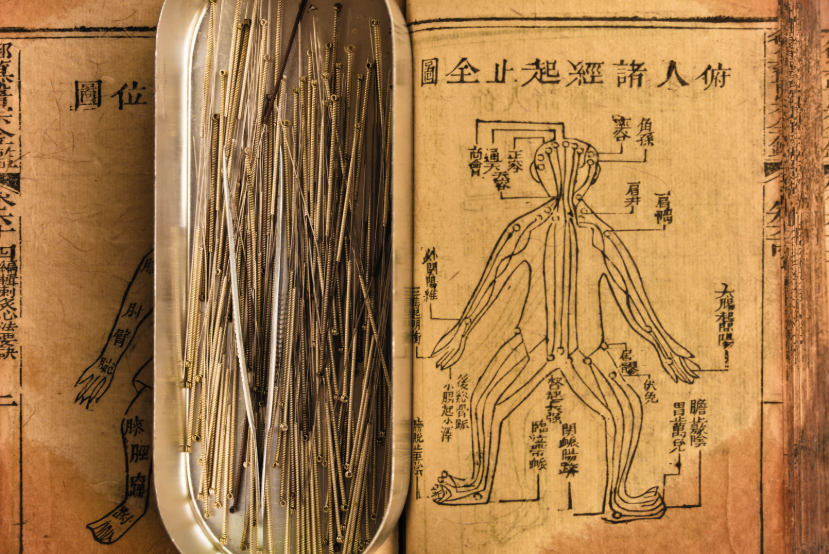
Acupuncture & Dry Needling Needles
Janet Travell, whose work on referred pain patterns forms the foundation of modern trigger point theory, was working with a hypodermic syringe and lidocaine ("wet needling") when she met Mark Seem, widely regarded as the father of physical medicine acupuncture in America. In 1990, when Travell was teaching alongside Maryland neurologist Robert Gerwin, Seem demonstrated his classical acupuncture approach to trigger point release using a thin solid filiform needle, a tool and technique neither had seen applied this way before. After that encounter, Gerwin sought out practitioners trained in the technique, which eventually opened the pathway through which dry needling entered physical therapy.
The lineage runs one direction. Dry needling did not inform acupuncture. Acupuncture informed dry needling.
On scope creep: What began as a tightly defined technique — needle in, needle out, no retention, targeting myofascial trigger points — has quietly expanded into an ever-growing menu: community dry needling, cosmetic dry needling, functional, homeostatic, and integrative dry needling. Most of these involve needling classical acupuncture points, sometimes using traditional point names, under the cover of new terminology. The further this expands from its original definition, the closer it gets to the practice of acupuncture.
It is also worth noting that in Pennsylvania, licensed acupuncturists are regulated by the State Board of Medicine, the same licensing body that oversees physicians, nurses, and physician assistants. This is not a fringe credential. It is a state-recognized medical license issued by the same authority that governs the practitioners dry needling proponents claim to be more scientifically rigorous than.
The patient safety concern is not theoretical. In December 2025, Pittsburgh Steelers linebacker T.J. Watt required surgery for a partially collapsed lung , a pneumothorax, sustained during a dry needling session at the team's practice facility. The credentials of the practitioner were never publicly disclosed. His teammate Patrick Queen, who prefers acupuncture, was direct in the aftermath: "One, you got to go to school for a longer period of time. There's a whole much more scientific thing that goes into it. I don't do the whole dry needle thing." Pennsylvania is one of the states where dry needling falls into a regulatory gray area for physical therapists. The incident happened here, in Pittsburgh, in our backyard.
The depth of the system
Where the frameworks diverge is in depth and in time. Chinese medicine represents thousands of years of continuous empirical observation, clinical refinement, and systematized inquiry into how the body responds to needle stimulus. No randomized controlled trial runs for two thousand years, but a clinical tradition that has survived, evolved, and remained internally consistent across that span is itself a form of evidence.
Classical texts described lymphatic-like drainage in the brain at a time when Western medicine did not formally identify the brain's glymphatic system until 2012, or confirm the existence of meningeal lymphatic vessels until 2015. They described the long uninterrupted fascial chains we now map with dissection, and the piezoelectric properties of connective tissue, one dimension of what was being captured by the term Qi. The pathways of spinal nerve distribution, the body's somatotopic organization, these were observed, systematized, and applied long before Western anatomy had language for them.
Dry needling operates from a peripheral model: find the taut band, needle the taut band, release the taut band. Its theoretical framework accounts for the local spinal reflex arc and the neurophysiological event of the twitch response, and that is legitimate as far as it goes. But that is also largely where it stops.
Acupuncture's somatotopic mapping reveals something categorically different. The body is represented in multiple overlapping maps, complete unto themselves, each one a system within the system. These microsystems exist throughout the body — on the ear, the scalp, the face, the hands, the feet — some running in conventional orientation, others inverted. A trained practitioner can work entirely within one microsystem and produce effects far from the site of needling. This concept has no equivalent in dry needling's framework and no explanation within a trigger point model.
Segmental relationships allow us to trace a peripheral symptom back to its spinal level and address it there. De qi, the characteristic propagated sensation of needle stimulation, represents activation of A-delta and C fibers with direct projections into descending pain modulation pathways. None of this is mysticism. All of it is applied neuroscience.
A practitioner working from a trigger point model alone is treating a shadow of the problem.
Acupuncture is a system for navigating the nervous system with a needle. Dry needling is a single technique borrowed from that system, stripped of its map.
A word about language
Channel theory is often where Western practitioners check out of the conversation. The language of rivers and Qi feels too distant from anatomy to take seriously, and the word "woo" tends to follow shortly after. It is worth pausing on that reaction.
Do you know what Western medical providers call the bottom of the spinal cord? The cauda equina. It sounds impressively medical, but it is Latin for "horsetail." The soleus muscle in the calf is named after a flat fish, for the way a fish fillet looks. And that tendon bundle on the inside of your knee, the pes anserinus, translates literally as "goose foot."
Western anatomy is full of colorful, observational language describing exactly what something looks like or how it behaves. We are comfortable with it because it comes to us in Latin and Greek rather than classical Chinese. The Western reading of Chinese medicine has followed the same arc as early Western ethnomusicologists encountering East Asian music — many assumed the scales were primitive, incomplete, somehow unresolved. What they were actually hearing was a sophisticated microtonal system that simply didn't conform to their expectations. The complexity was always there. The listener lacked the framework to recognize it.
So before dismissing Qi or "fish-bite response" as unscientific, it is worth examining the bias we bring to whose descriptive language we accept as legitimate — and whose we don't.
The anatomy of the channels
What looks like metaphor from the outside is, on closer examination, a remarkably precise observational system expressed in the language available at the time.
The channels follow spinal nerve territories, dermatomal and myotomal distributions, with a consistency that is difficult to attribute to coincidence. They track the long uninterrupted fascial planes that Tom Myers mapped in the late twentieth century as Anatomy Trains, planes that classical Chinese medicine had already systematized centuries earlier. Primary channel points cluster at sites where nerves, vessels, and connective tissue converge. What we now recognize as neurovascular bundles.
This is no longer simply a theoretical argument. Neuroanatomist and acupuncturist Poney Chiang has been conducting cadaveric dissection research demonstrating that primary acupuncture points occur consistently at nerve bifurcations and nerve trunks. His findings are published on PubMed and represent some of the most rigorous anatomical validation of channel theory currently available. The points were never arbitrary. We are only now developing the dissection technology precise enough to see what classical practitioners had already mapped by hand.
The muscle fasciculation that dry needling practitioners call a "twitch response" has been documented in Chinese medical literature for two thousand years. Classical texts describe it as the "fish-bite" response, the sensation of the muscle grabbing the needle likened to a fish nibbling on a line. The technique is not borrowed from physical therapy. The language is simply newer.
At Heal, our practitioners draw from multiple styles because patients are not uniform in how they respond. Some do better with a direct orthopedic approach, needling into the affected tissue. Others respond more profoundly to distal channel work, where the needle never goes near the site of pain at all. In channel theory, a distal point is always a local point to where you are working. The geography is simply larger than a trigger point model allows for. The ability to move fluidly between these approaches is not a sign of an inconsistent system — it is a sign of a sophisticated one.
It takes four or five neuroanatomical concepts working in combination to approximate what channel theory describes as a unified system. That isn't a limitation of Chinese medicine. It's an indication of how much ground it was covering.
The system was never primitive. It was just written in a language Western medicine is still learning to read.
Selected references
Finando & Finando (2012). Qi, acupuncture, and the fascia. Journal of Alternative and Complementary Medicine. PMID 22874011
Yi & Encong (1996). Acupuncture treatment and the piezoelectric effect. European Journal of Oriental Medicine.
Langevin & Yandow (2002). Relationship of acupuncture points and channels to connective tissue planes. Anatomical Record.
Iliff et al. (2012). A paravascular pathway facilitates CSF flow through the brain parenchyma. Science Translational Medicine.
Louveau et al. (2015). Structural and functional features of central nervous system lymphatic vessels. Nature.
Chiang, P. Cadaveric dissection research on acupuncture point neuroanatomy. Available via PubMed.
Myers, T. (2001). Anatomy Trains. Churchill Livingstone.
Seem, M. (2015). Public comment to the Virginia Board of Physical Therapy. Comment ID: 47915.
McIntyre, A. (2016). Dry needling is acupuncture, but acupuncture is not dry needling. Washington East Asian Medicine Association.
Pryor & Bell (2025, Dec 13). T.J. Watt's collapsed lung injury update. ESPN.